HCG 5000iu – Human Chorionic Gonadotropin – Gonase
HCG – Human Chorionic Gonadotropin
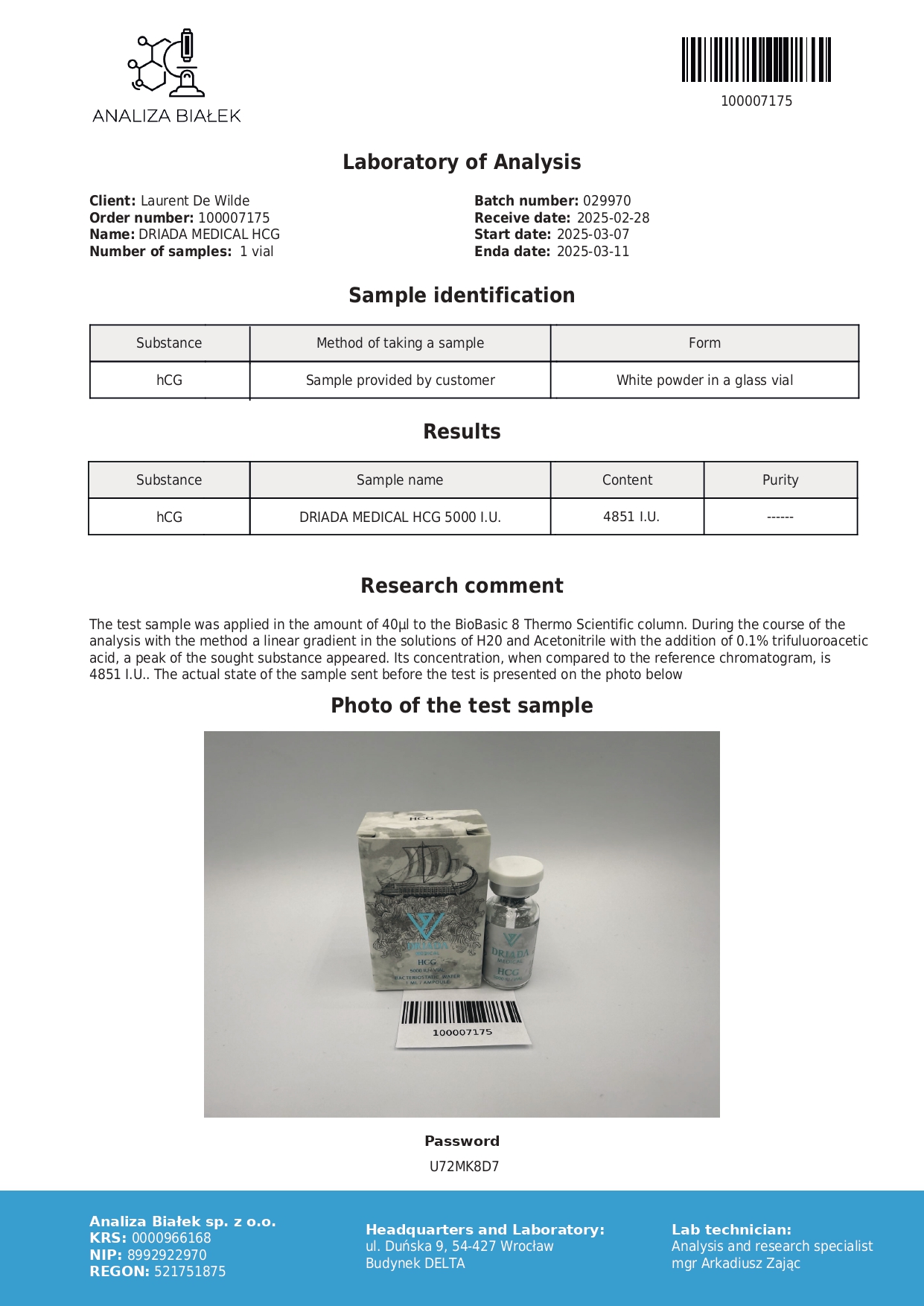
HCG – Human Chorionic Gonadotropin
Composition: human chorionic gonadotropin (HCG) 5000 IU.
Category: peptide, hormonal support during and after the cycle.
Purpose: stimulation of gonadal activity, maintenance of endogenous testosterone production, and support for the recovery of reproductive function.
Form: vial containing lyophilized powder + 1-ml vial of water for injection for reconstitution.
Administration: subcutaneous injection.
- Shipping (if the product is in stock): 3 business days for processing and 5 to 20 business days for shipping
- Processing and shipping costs: €27 throughout Italy
What is hCG (Gonase)?
Human chorionic gonadotropin, commonly referred to as hCG and also marketed as Gonase, is a peptide hormone produced naturally during pregnancy. In sports and clinical settings, it is used to maintain and restore endogenous testosterone production when the hormonal axis is suppressed, for example during cycles of anabolic steroids (AAS).
hCG/Gonasem acts on luteinizing hormone (LH) by binding to its receptors in Leydig cells and stimulating testosterone synthesis. In medicine, it was initially used to induce ovulation in women and support spermatogenesis and fertility in men; it has since become a mainstay of hormonal support for athletes.
Main effects of hCG (Gonase)
- 📈 Maintains and increases endogenous testosterone during AAS suppression
- 🧬 Supports fertility and libido
- ⚙️ Preserves testicular volume and function, preventing atrophy
- 🔁 Helps hormonal balance during prolonged cycles
How to take hCG (Gonase)
Before use, ask for instructions on reconstitution and injection technique. hCG is particularly recommended for cycles longer than 6 weeks.
Typical diagram
| Scope | Dosage | Frequency | Duration |
|---|---|---|---|
| During AAS cycle (from week 4) | ~1000 IU/week (750–1250 IU) | 2 injections of 500 IU | Until the end of the cycle |
| Libido/energy support | 500 IU | 1–2 times a week | 2–4 weeks |
📌 Monitor: total/free testosterone, LH, FSH, estradiol, prolactin; in long cycles, also β-hCG
Precautions
- Do not combine SERMs (clomiphene, tamoxifen) with hCG; reserve them for PCT
- Avoid combining with other gonadotropins or LH mimetics.
- Watch out for signs of excess estrogen (edema, nipple sensitivity).
- Use moderate doses to avoid desensitization of LH receptors.
Possible side effects
- Increased estrogen (with overdose)
-
Testicular tenderness or swelling
-
Mood swings, fatigue
Storage
-
Refrigerator at 2–8 °C, protected from light and heat
-
After reconstitution: 1–2 months if stored properly
How hCG (Gonase) works
hCG is a “functional duplicate of LH”: it maintains intratesticular testosterone (ITT) and gonadal function even when the HPG axis is suppressed by AAS. For this reason, it is ideal during the cycle, whereas during PCT, it is preferable to reactivate the upper branch (hypothalamus/pituitary) with SERMs
Clinical studies (Coviello 2005; Roth 2010–2011) show that low–moderate doses of hCG maintain ITT at near-physiological levels with a dose-dependent response up to the threshold, confirming the importance of avoiding excesses.
Quick FAQs
- When to start? Around week 4 of the AAS cycle.
- During PCT? No, stop first and switch to SERMs.
- Fat loss? Indirectly, yes, by supporting testosterone, energy, and lean mass.
Related products
-
Nolvados 10 mg (Tamoxifen Citrate) – Nolvadex
The original price was: $34.25 €The current price is: €25. -
Propios 100 mg/ml (Testosterone Propionate)
The original price was: €46.41 €The current price is: €41. -
Trenentos 200 mg/ml (Trenbolone Enanthate)
The original price was: €63.58 €The current price is: 58 €. -
Cypilos 250 mg/ml (Testosterone Cypionate)
The original price was: $42.39 €The current price is: €39. -
Raloxos 30mg (Raloxifene)
The original price was: €32.29 €The current price is: €29.